Failure Mode Effects & Criticality Analysis (FMEA/FMECA)
Failure Mode Effects & Criticality Analysis (FMECA) is a structured and proactive risk assessment tool used to identify potential failure modes within a system, product, process, or service, evaluate their effects, and prioritise them based on risk. An extension of Failure Mode and Effects Analysis (FMEA), FMECA adds a criticality assessment by calculating a Risk Priority Number (RPN) using the likelihood of occurrence, severity of impact, and detectability of the failure. The method enables organisations to anticipate problems before they occur, improve safety and reliability, and focus resources on the highest-risk areas. FMECA is widely used in engineering, manufacturing, aerospace, healthcare, quality management, and operational excellence programmes.
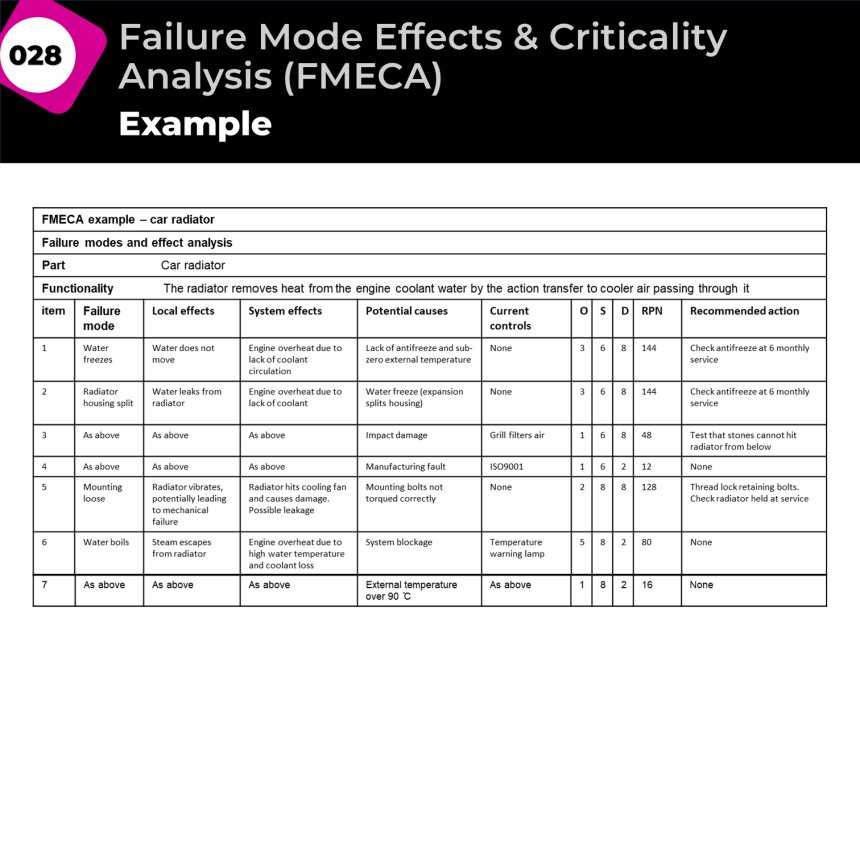
Failure Mode Effects and Criticality Analysis (FMECA) begins by clearly defining the system, process, product, or service that will be analysed. The objective is to understand where failures could occur and what impact those failures may have on customers, operations, safety, quality, or business performance. To make the analysis manageable, the system is broken down into smaller components, subsystems, or process steps. Each component is then reviewed to understand its intended function and role within the overall system.
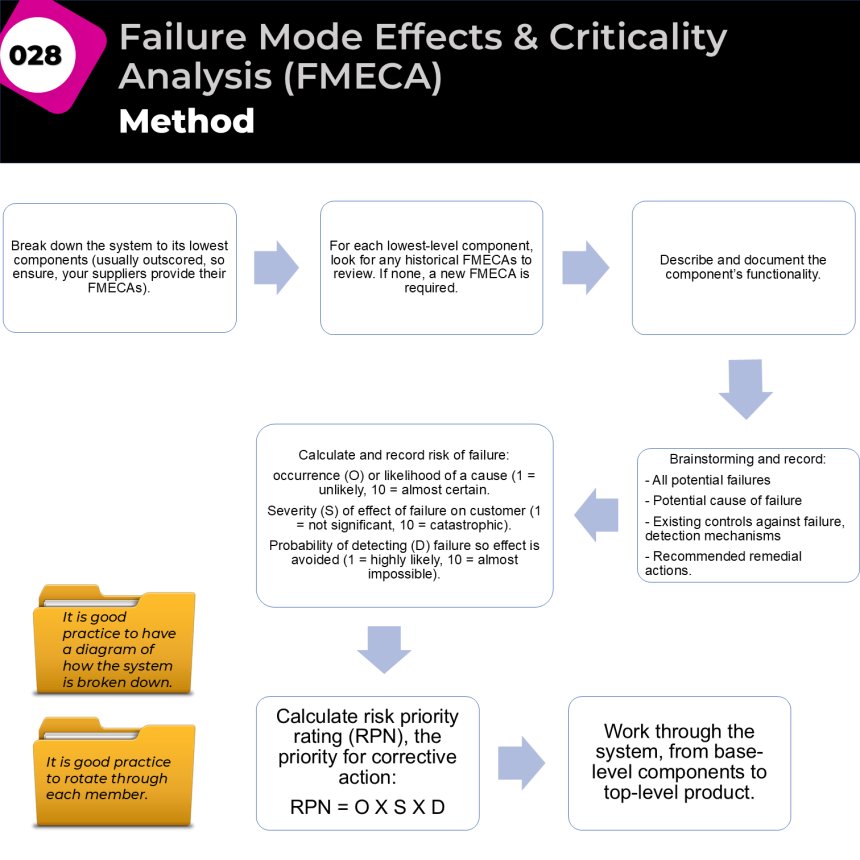
The team then conducts a structured brainstorming session to identify all potential failure modes for each component. A failure mode is simply a way in which the component could fail to perform its intended function. For every failure mode identified, the team examines the possible causes of failure, the likely effects of the failure, and any existing controls or detection mechanisms already in place to prevent or identify the problem. This ensures a comprehensive understanding of both the risk and the organisation's current ability to manage it.
Next, each failure mode is assessed using three criteria. Occurrence (O) measures how likely the failure is to happen. Severity (S) evaluates the impact of the failure if it occurs. Detection (D) assesses how likely it is that the failure will be detected before causing harm or disruption. Each factor is typically scored on a scale from 1 to 10. These scores are then multiplied to calculate the Risk Priority Number (RPN):
RPN = Occurrence × Severity × Detection
The higher the RPN, the greater the priority for corrective action. Failure modes are ranked according to their RPN scores, allowing the team to focus resources on the most significant risks first. Corrective and preventive actions are then developed and implemented to reduce the likelihood, impact, or detectability of the failure. Once improvements have been made, the FMECA is revisited and rescored to confirm that the risk has been reduced to an acceptable level.
Example
Consider a manufacturing company experiencing frequent breakdowns of a critical packaging machine. The FMECA team breaks the machine into key components such as the conveyor system, sensors, motors, and control panel. During the analysis, the team identifies a potential failure mode: sensor failure causing incorrect product detection.
The team determines that the failure may be caused by dust accumulation on the sensor lens. The effect of the failure is production stoppage, delayed deliveries, and customer dissatisfaction. Existing controls consist of monthly cleaning and operator visual inspections. The team assigns the following scores:
- Occurrence (O) = 7 (fairly common)
- Severity (S) = 8 (significant operational disruption)
- Detection (D) = 6 (moderate chance of detection)
The resulting RPN is:
RPN = 7 × 8 × 6 = 336
Since this is a high-risk score, the team decides to implement additional controls, including weekly sensor cleaning, automated sensor diagnostics, and preventive maintenance alerts. After implementation, the scores are reassessed:
- Occurrence (O) = 3
- Severity (S) = 8
- Detection (D) = 2
The new RPN becomes:
RPN = 3 × 8 × 2 = 48
This significant reduction demonstrates that the risk has been effectively mitigated. Through FMECA, the organisation proactively prevents future failures, improves equipment reliability, and reduces the likelihood of production disruptions.
Best Used When
FMECA is most effective when organisations need to proactively identify and mitigate risks before failures occur. It is particularly valuable during system design, process development, product development, equipment reliability reviews, safety assessments, and major improvement projects. The method is especially useful for high-risk operations where failures could result in significant financial loss, safety incidents, quality issues, regulatory non-compliance, or customer dissatisfaction.
Typical Applications
- Product and process design reviews.
- Manufacturing and production systems.
- Safety-critical operations.
- Engineering and maintenance planning.
- Healthcare and patient safety systems.
- New equipment commissioning.
- Operational risk management.
- Reliability and quality improvement initiatives.
Key Benefits
- Identifies potential failures before they occur.
- Prioritises risks using an objective scoring method.
- Improves product, process, and system reliability.
- Enhances safety and regulatory compliance.
- Supports better design and operational decisions.
- Reduces downtime, defects, and operational disruptions.
- Focuses improvement resources on the highest-risk areas.
- Strengthens cross-functional collaboration.
- Encourages preventive rather than reactive management.
- Improves customer satisfaction through greater reliability and quality.
JSSB Practitioner Note
FMECA is often best applied after initial root causes have been identified through tools such as Five Whys and Fishbone Analysis, and before implementing corrective actions. It answers a different question:
- Five Whys: Why did the problem happen?
- Fishbone: What factors may have contributed?
- FMECA: Which potential failures pose the greatest risk and should be addressed first?
This makes FMECA a powerful bridge between Root Cause Analysis and Risk-Based Decision Making.
Files
Share
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Angry
0
Angry
0
 Sad
0
Sad
0
 Wow
1
Wow
1